Life
The Killer Belly
Many Indians have it. But do they know it's a possible death warrant?
|
Here’s a life-or-death test for you.
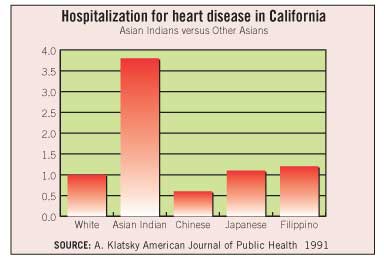
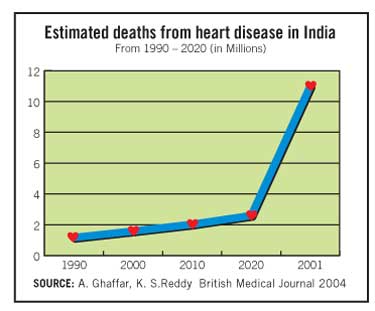
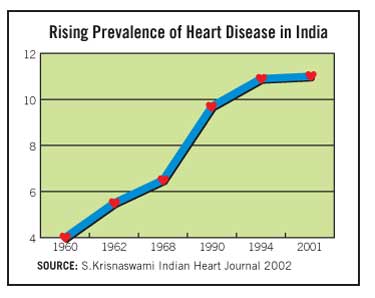
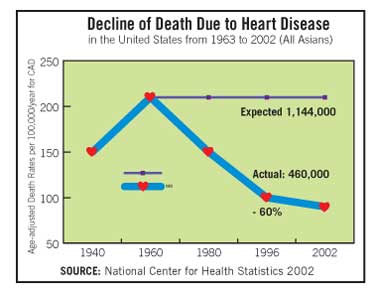
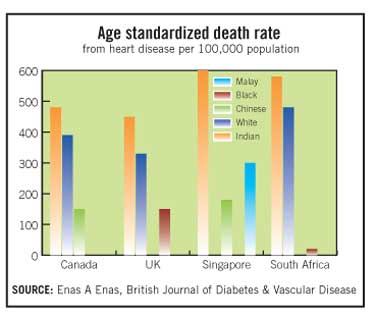
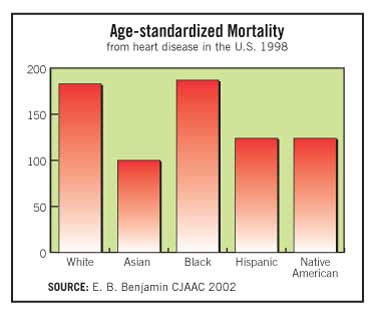
Pick up a tape measure. Wrap it around your waist at navel level. If you’re an Indian woman and measure more than 32 inches or an Indian man over 35 inches, brace yourself. Within the next 10 or 20 years you are almost certain to get diabetes or heart disease – or both. While heart disease declined 60 percent in the last 30 years in the United States, it has escalated by 300 percent in India. U.S. studies have found that Indians in the United States have three to four times the heart disease rate of the mainstream U.S. population. Another study by the HMO Kaiser Permanente in California found that hospitalization rates for heart surgery among Indian Americans is four times that of the mainstream population.
While 60 percent of heart attacks amongst Americans occur after age 55, nearly half of all heart attacks among Indian men strike under the age of 55 and 25 percent under the age of 40. Indian women share these high rates of heart disease. Thousands of Indian American men in their 40s and 50s succumb to a first, fatal heart attack every year.
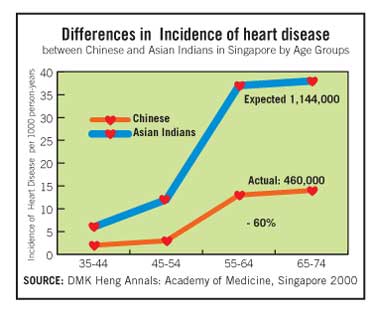
“Every population gets heart disease and diabetes, but Indians get more of it and get it at least ten years earlier,” says Dr. Enas A. Enas, Director of the Coronary Artery Disease among Asian Indians (CADI) Research Foundation and Advanced Heart Lipid Clinic in Downers Grove, Ill, and a clinical associate professor at the University of Illinois at Chicago. Enas, who has done pioneering research on heart disease among Indians during the last 15 years, is author of more than 50 articles published in major cardiology journals. He not only was among the first to sound the alarm on the high rate of heart disease amongst Indians in the United States, but also reported the high levels of lipoprotein (a) – a genetic variant of LDL cholesterol among Indians and its crucial role in the high rates of pre-mature heart disease among the Indian population. The research at the CADI Research Foundation shows that abdominal obesity is two to three times more common among Indians than in general obesity measured by BMI (Body Mass Index). Fat around the waist and abdomen is the most dangerous fat for cardiovascular and diabetic risk, compared to fat in thighs and buttocks. The problem with the big belly is that visceral fat serves as an active chemical factory, producing biological and active molecules and hormones that lead to the development of diabetes and heart disease. Weight control is crucial because Indians get diabetes and heart disease even though they are 30 pounds lighter than mainstream Americans. So not only do Indians get heart disease earlier than the rest of the population, they get it at weights 30-40 pounds lower than the others. Enas says the traditional BMI measures don’t apply to Indians.
The most significant measure is the waistline. Even children as young as 8 years old in the UK showed a propensity for diabetes and high cholesterol as their waistline increased. For an Indian child, Enas says, the abnormality is double that of a white child, because of the different distribution of abdominal obesity and general obesity. Few physicians know of this Indian paradox and because the relative size of the population is small (under 1 percent of the national) these facts have not registered in mainstream research. Few survivors are willing to discuss their experiences, so not only is heart disease a silent killer, but there is also a deafening silence about its widespread prevalence within the Indian community.
Rajan (name altered at request), a business executive in New Jersey with two children, had his world turned upside down when he, suffered a heart attack at age 35. He was a heavy smoker, in a stressful job and had a family history as several uncles died before the age of 45. Both his father and brother died in their 50s. Yet his doctors ruled out heart disease, because of his young age. They gave him several tests for shortness of breath, including a stress valium test, all of which proved negative. So when he started throwing up one night, heart problems were the last thing on his mind. He assumed he was suffering from food poisoning. His wife and children were away in India, but his brother called 911 and the ambulance whisked him away to the hospital. In the emergency room doctors found that four of his arteries were blocked and he had to undergo quadruple bypass surgery. Rajan’s life changed overnight and he gave up his sedentary lifestyle, drinking and stressful job. He quit smoking cold turkey, because his surgery, he says, was like “shock therapy”; he knew his life depended on it. Fifteen years later he is vigilant about his health and plays by the rules. Sudesh Kannan took preventive steps to avoid becoming the same casualty. Just six months after he entered school in IIT Madras, his father, who was diabetic, died of a heart attack. A joyous time turned traumatic for the 19-year-old. He recalls that another three students in his batch also lost their fathers to heart disease during that time. Kannan came to Madison, Wisc., for his masters from the University of Wisconsin. After completing his PhD at the University of Virginia, he got a job as an engineer and settled in North Carolina. He was just 35 when a routine check up in his doctor’s office showed he had very high cholesterol and triglcerides, even though he was quite thin. He says, “I thought, my father had died young and I don’t want to die young. I tried to exercise and went on a completely vegetarian diet, but it was not helping lower my cholesterol level at all.”
“We are in a prosperous country, right?” he says. “So we can get unlimited amounts of food, but we have to realize we have to eat the right amount of food and the right kind. I cut down my rice and rotis and added fruit and vegetables. When I ate it in the right combination I found I had this unlimited source of energy and could run marathons, I could bike. My thinking style became clearer, there was no sluggishness.” And here we return to the killer belly. Says Kannan, “I was not overweight when you looked at me, but I had a big paunch. Indians may look skinny, but we have big paunches. I dropped just ten pounds but my stomach went flat. So you know there’s a connection basically. I had the classic combination – and if I hadn’t taken care of myself I would have been a diabetic by now.”
Dr. Naras Bhat, author of Reversing Heart Disease and Preventing Cancer, is a noted cardiologist in private practice in San Francisco and has seen over 295 South Asian patients in his practice. Along with several other physicians, he is on the Physician Advisory Committee of the newly created South Asian Heart Center at El Camino Hospital in Santa Clara in Silicon Valley, which is home to many Indian IT professionals. The Center’s mission is to dramatically reduce the high incidence of coronary artery disease among South Asians through a comprehensive, culturally appropriate program, incorporating education, advanced screening, lifestyle changes and case management. He says that genetically all the people of the subcontinent have common indicators of impending heart disease and diabetes. “We quickly develop abdominal obesity and that leads to the condition known as metabolic syndrome, whereby your triglycerides and small, dense LDL, the worst part of bad cholesterol, goes up, while HDL2B, the best part of your good cholesterol, goes down.” He adds, “With abdominal obesity, insulin resistance increases and so you have more insulin circulating in the body. As a result, it’s a vicious circle and you end up depositing more fat on your belly. To add fuel to the fire, a sedentary lifestyle and stress makes the situation even worse.”
Abdominal obesity is something that Dr. Valavanur Subramanian, a noted cardio surgeon, also cautions against. Subramanian, who was named one of New York’s best doctors by New York magazine, is chairman of the Cardiothoracic Surgery department at Lenox Hill Hospital in New York. Since 1995, he has developed various innovative techniques for minimally invasive and beating heart coronary bypass surgery, and with his colleagues is working on robotic heart surgery. He sees many Indian patients and says waist girth is is greatest concern. “Especially if your abdominal weight is increased, it co-relates with the fact that you may have underlying diabetes or coronary heart disease,” he says. “If people do not have an active lifestyle that also gives rise to abdominal obesity. If someone has an increased abdominal girth and has not been to a doctor, he should check his blood sugar, and he should go to a primary care doctor or cardiologist to figure out if he has coronary heart disease.” He points out that Indians have a far higher rate of diabetes than other nationalities. Since there is a high co-relation between diabetes and heart disease, Indians have to take special care. He says, “We do have a very high carbohydrate intake, we do eat a lot of rice. Many Indians tend to have a mild form of diabetes and rice tends to exaggerate that.” He suggests cutting down on oil, carbohydrates and sugar and turning to a high protein diet and vigorous exercise.
Bhat says all aspects of the tripod or three legged model of heart disease need to be treated: the plumbing or blockage of arteries, the chemicals like cholesterol and the emotional aspect, such as anger, depression and stress. Curiously enough, there are cultural factors too for the high incidence of diabetes and heart disease among South Asians. Enas says cultural mores, such as arranged marriages within caste and sub caste and socio-economic parameters, contribute to the Indian propensity for heart disease. Gene abnormalities are magnified through such relationships, increasing the genetic predisposition to heart disease. In fact, one of the major reasons for early heart disease amongst Pakistanis is the practice of arranged marriages within close family, as this increases the chance of gene abnormality. Heart disease often comes without major symptoms. In the 1990s, Vijaya Benjamin of Chicago went to India to celebrate his daughter’s wedding, but ended up with his first heart attack, immediately after the festivities. Since he had normal cholesterol levels, the attack was blamed on stress. Back in Chicago, he had to have coronary quadruple bypass surgery and was found to have an abnormal level of lipoprotein a. Benjamin, who worked in a diagnostic service, says he has a family history of heart disease, but had never watched his diet. When he came to the United States from Trivandrum 30 years ago, he was just 128 pounds and in the course of the first year he gained 40 pounds living off fast food, smoking, and pursuing a sedentary lifestyle.
After his bypass surgery he is a changed man and has maintained an active lifestyle for 10 years: “I’ve quit smoking, I have only home food and I go for cardiac rehab exercises three times a week.” After his experience, he says, his colleagues at work have also started going for walks and exercise. Meanwhile Kannan, who had moved from North Carolina to Chicago, contacted Enas who had helped him get on the path to better health. He recalls, “His house was on the way to the temple and I passed it every time I visited the temple.” The two men finally met and decided to collaborate on a book about heart disease in layman’s language to get the message out to South Asians. The result was the just published book, How to Beat the Heart Disease Epidemic Among South Asians: A Prevention and Management Guide for Asian Indians and their Doctors. Out in Houston, Texas, Anil Kapoor also had a family history of heart disease and some distressing moments led him to double bypass surgery at the age of 50. Kapoor, who is from Allahabad, came to the United States 30 years ago and is a shipping executive. In 1986 he had agina and a stent was inserted. He says, “I read up and I thought I was doing good things on my own, but I don’t think I was.” He had pre-heart attack symptoms and a cardiologist told him he needed bypass surgery. Kapoor says, “My view is that we Indians are very susceptible to heart disease, because of our lifestyle, our food, our culture. I had not been paying much attention to the food. The weight was not what it should have been and the exercise was not enough.”
He changed his lifestyle after the bypass. Did he have to slow down? He says, “No, that’s a wrong idea. You never slow down after bypass surgery. You need to be more active. Relatives in India say they have heart problems so they can’t do anything. But that is absurd. I love fried food, but I don’t eat it now. I do treadmill five days a week at 4/5 miles per hour every morning. I walk the nine holes of golf three to four times a week. I’ve maintained my weight since the last 10 years. Every six months I go for a cholesterol check up and stress test.” He adds, “I get upset when people say ‘Oh, I’m doing yoga and not taking too much of ghee.’ We Indians are not like Americans. We do not exercise, all we do is take a stroll in the evening, and that stroll I call ‘Jhanwase ki chaal’ – or the relaxed walk of the bridegroom and the baraat! That’s not going to cut it. To lose weight you have to pump your heart. You have to burn more calories than you take in. Yoga is good, but it’s not going to make you lose weight.” From his experience, he says, it’s necessary to change the Indian cooking style. Instead of deep frying, he sautés onions in Canola oil and then adds water and masalas. He says, “For the last five years I have given up rice, chappatis, bread and potatoes, and emphasize vegetables and fish. I eat a lot of fruit. My wife says I eat fruits like a meal.”
Indeed, for those with heart disease and diabetes, a huge life change is mandatory, but it can be taken in little steps. Madhuri Mathur of Long Island knows the tribulations of trying to follow the rules Her husband, Madan Mohan discovered his major heart problem quite by accident when she asked him to accompany her during a checkup and since they had the same primary care doctor she convinced him to have an EKG too. The results raised flags and Mohan was sent for a stress test and an angiogram. Most people are not happy at such news and her husband jokingly told her, “All my life I listen to you. This is the last time! See what happened!” He had to undergo an angioplasty since three of his arteries were totally blocked and he also needed open-heart surgery. Yet, he had experienced no pain or symptoms to signal that his heart was in such trouble. Mohan had been a diabetic all his life and his mother was one too. People with diabetes are especially prone to heart disease, but many don’t see the connection. Now Mohan takes prescription medicines for his health problems and also uses the treadmill regularly. At 74, he’s taken charge of his health. Madhuri Mathur came to New York from Delhi after staying some years in Kabul, Afghanistan. At that time she was just 30 and had two small children. She became diabetic in 1999 and both her mother and grandmother had diabetes. A good cook, she was into entertaining and eating out socially. Mathur discovered she was diabetin also by accident. She tended to get thirsty and drank water all the time. Her daughter insisted she check her sugar level, which she did on her husband’s Glucometer. The figure was a whopping 500! She thought the instrument was faulty, but a visit to her doctor confirmed that she had diabetes. For Mathur, who is a vegetarian, “being good” is harder, as it is for many people used to the Indian food habits. Now that mithais are available freely here, she says, she has stopped making them at home, but cannot resist the ready products just waiting to be brought home. She also finds it hard to turn away from rice and rotis, which people with diabetes have to avoid. “I love chole bature, but I had to cut that down,” she says regretfully. “Everything is paired with carbs – rajma chaval, curry chaval and so I have had to cut them out. But I find it hard to cut out the potatoes, because all the sabzis require it – alu baigan, gobi alu, even cabbage. I used to put four potatoes, but now I put only one. I cannot stop it, but I can cut down like that.” Weight loss is crucial for people with heart disease and diabetes, but exercise often is a problem for an aging population afflicted with arthritis. Mathur had to give up her walks due to knee problems, but now has a spiffy new treadmill, thanks to her daughter who is a therapist. So her daughter must be guiding her on health issues? “Yes, she’s guiding me, but it depends on how much I’m listening,” says Mathur. “She gives me so many exercises which she says are easy, but I say, ‘Theek hai, kal karloongi, kal karloongi. (Okay, I’ll do them tomorrow.)” Dr. Tara Shani, an internist in private practice in Houston, Texas, has seen many Indian patients who suffer from heart disease and diabetes. “They are basically in denial. Many have high blood pressure, high cholesterol, diabetes and heart disease, and they don’t watch their diet, they eat what they want, and they get very little exercise. Their compliance is very poor and they don’t really understand the disease or its complications. You really have to pin it down to them and they’ll take the medicines, but with a lot of reluctance. I don’t see active participation, like watching their diet or doing exercise.” She finds resistance to making lifestyle changes, like giving up smoking, losing weight or controlling alcohol. But don’t they realize the seriousness? “They do,” she says of the large South Asian community. “However, I think there’s a denial. They don’t like to be labeled, so they don’t want to acknowledge they have a problem. When you don’t acknowledge you have a problem you’re not going to treat it.” Often she finds Indians will seeks ways to avoid taking the prescribed medicine, turning to ayurveda or homeopathy or eating foods that they’ve been told help their diabetes. Only when they experience a severe health setback do they turn to the medications. Even though most Indians are highly educated, she attributes their inhibitions to cultural factors. “They tend to stay away from taking medication. They’ll take the prescription, they’ll put it in their bags, but in follow up visits you learn they haven’t taken the prescribed medicines.” Enas says Indians also have a psychological obstacle in their misguided view of karma and that everything is pre-ordained. “If you get diabetes, or heart disease and you put it on karma – that doesn’t leave any room for action,” he says. “When we want to send our kids to the best schools, we don’t leave it to karma, we push to the maximum. But when it comes to our own health, we leave it to karma. So the concept of prevention does not exist, even though heart disease and coronary artery disease have now become the most predictable, the most preventable and most treatable of all chronic diseases.” “Going into the pool with other people was a big step for me. I had never worn a swimsuit or even shorts,” she recalls. “I was saying to my daughter-in-law, ‘Oh, my god, other men are in the pool. How are we going in the same pool?’ She told me, ‘Mummyjee, it’s OK, but I said ‘For me going in a swimsuit. no, no!’ So I wear a tee shirt and shorts in the pool. Even putting on shorts and going into the pool is a big change and a big compromise from my side.” She adds with a laugh, “See, in our culture, we can show our tummies, but not our legs! It’s the reverse from here, where they are showing their legs, but cannot show their tummy!” Yes, even small, seemingly inconsequential changes often require courage, but yield dramatic results. Sudesh Kannan, whose father died of a heart attack many years ago, tried to rewrite his destiny and work at ridding himself of the killer belly. His changed lifestyle and the foods fed to the family by his nutritionist wife Akila have been a big influence on their children, Vinesh, 9 and Pavan, 3. On a visit to Disney World, the Mickey Mouse character asked Vinesh for his favorite food. Vinesh, then 5, promptly and enthusiastically replied, “Broccoli!” Children are savvy. They follow not what you say, but what you yourself do. Says Kannan: “That’s exactly right. And you have to integrate right eating and exercise into your daily life. When we go hiking, I carry my younger son in a backpack, and when my elder son goes biking, I run alongside him.” “If you don’t have a family history of heart disease or diabetes, and you drink, smoke or are obese, yours is a manmade history,” says Enas. “Genetics loads the gun, environment pulls the trigger. So if you get heart disease, don’t blame your parents and grandparents. Do something.”
|






You must be logged in to post a comment Login